Risk Factors: What They Are and Why They Matter in Medicine
Dr. Marco De Nardin
Medical Doctor, Specialist in Anesthesiology, Intensive Care and Pain Management
Not every patient with the same risk factors gets sick. Not everyone without risk factors stays healthy. And yet risk factors are one of the most powerful tools in modern medicine: they let us identify who is most vulnerable, intervene before disease appears, and personalize surveillance plans. Understanding what they are — and what they are not — is essential to using them correctly.
What Is a Risk Factor?
A risk factor is any characteristic, condition, or behavior that increases the probability that a person will develop a given disease. The technical definition comes from epidemiology: we speak of a risk factor when population studies demonstrate that those exposed to a given characteristic develop the disease more frequently than those who are not.
One crucial point to clarify right away: a risk factor is NOT a cause. It is a statistical condition that makes an event more likely, but it does not determine it with certainty. Having hypertension (high blood pressure) is a risk factor for stroke, but thousands of people with hypertension will never have one. Not having hypertension lowers the risk but does not eliminate it: strokes also occur in people with normal blood pressure. The link between a risk factor and disease is probabilistic, not deterministic. The distinction between a risk factor and a cause lies at the heart of etiology — the branch of medicine that studies the causes of disease.
Knowing your own risk factors is the prerequisite for acting on them — and the prerequisite for prevention.
Modifiable and Non-Modifiable Risk Factors
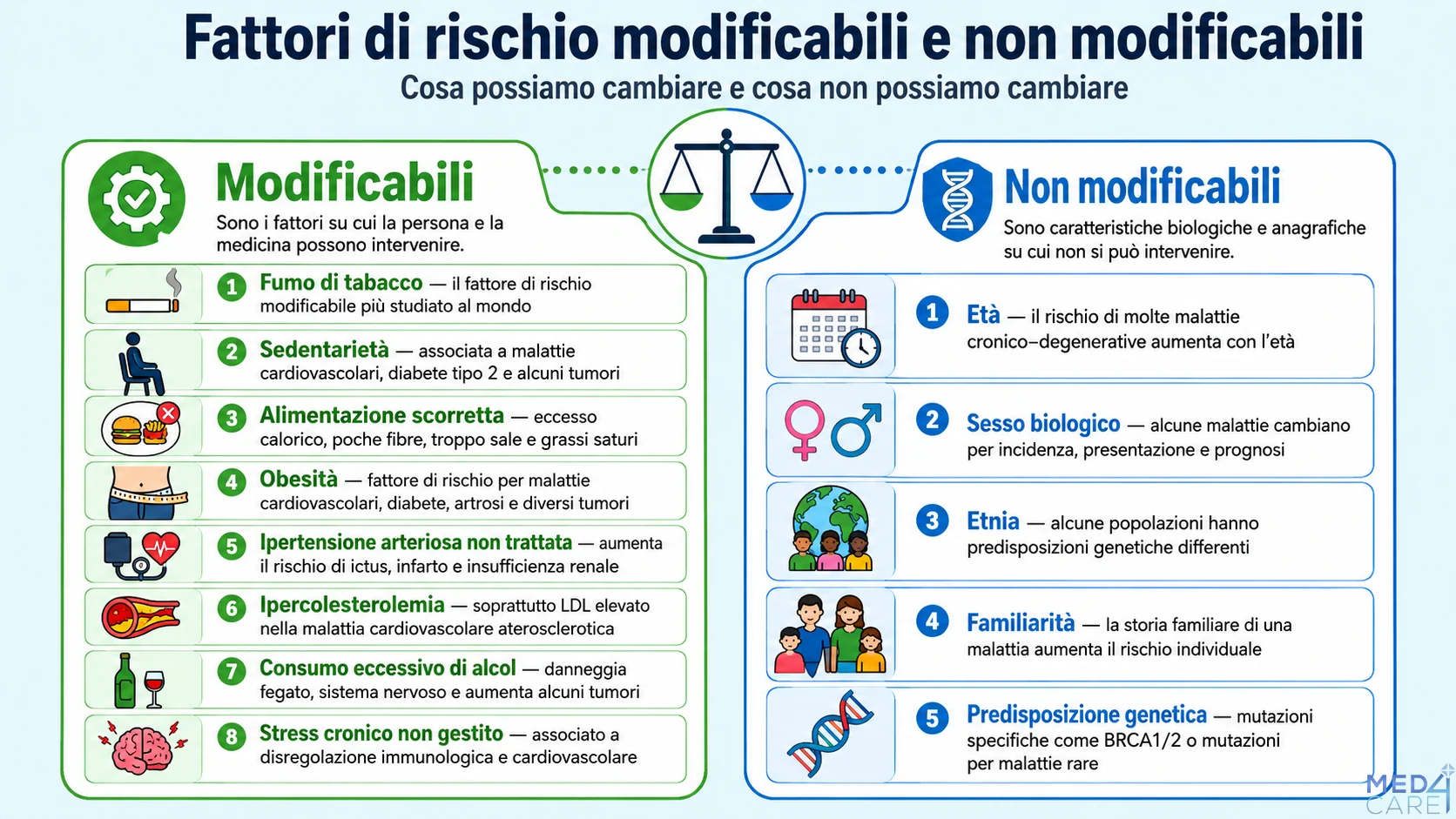
The most important distinction in preventive medicine is between factors we can change and factors we cannot change.
Modifiable risk factors are those that the individual and medicine can act upon:
Tobacco smoking — the most studied modifiable risk factor in the world
Physical inactivity — associated with cardiovascular disease, type 2 diabetes, and certain cancers
Poor diet — leading to excess calories, low fiber intake, and too much salt and saturated fat
Obesity — an independent risk factor for cardiovascular disease, diabetes, osteoarthritis, and several cancers
Untreated hypertension — a major risk factor for stroke, heart attack, and kidney failure
High cholesterol — particularly elevated LDL in atherosclerotic cardiovascular disease
Excessive alcohol consumption — damages the liver and nervous system and contributes to certain cancers
Unmanaged chronic stress — associated with immune and cardiovascular dysregulation
Non-modifiable risk factors are biological and demographic characteristics that cannot be changed:
Age — the risk of almost all chronic degenerative diseases increases with age
Biological sex — some diseases differ in incidence, presentation, and prognosis between men and women
Ethnicity — some populations carry a different genetic predisposition to certain diseases
Family history — a family history of a disease increases individual risk
Genetic predisposition — specific mutations (BRCA1/2 for breast cancer, mutations linked to rare diseases)
Preventive medicine acts on modifiable factors by trying to reduce or eliminate them. It monitors non-modifiable factors in order to intensify surveillance in the people who have them.
How Risk Is Measured: Key Concepts
Risk factors are not all equivalent: some increase risk substantially, others only slightly. Specific statistical measures are used to quantify this increase.
Relative risk (RR) expresses how many times more likely an event is in those exposed to a risk factor compared with those who are not. A smoker has a relative risk of developing lung cancer 15–30 times higher than a non-smoker (RR 15–30). That is an enormous effect. By comparison, hypertension increases the risk of stroke roughly 3–4 times (RR 3–4) — significant, but far smaller.
Absolute risk is the concrete probability that a person will develop the disease over a given period. Relative risk alone can be misleading: an RR of 3 applied to a disease that affects 1 person in 10,000 still yields a very low absolute risk (3 in 10,000). An RR of 1.5 applied to a disease that affects 1 in 10 yields a far more meaningful absolute risk (1.5 in 10). In clinical communication, absolute risk is almost always more useful than relative risk.
The NNH (Number Needed to Harm) completes the picture: how many people must be exposed to a risk factor for one of them to be harmed. The lower it is, the more dangerous the factor.
Risk Factors in Major Diseases
Three concrete examples illustrate how risk factors combine in practice:
Cardiovascular disease: smoking, hypertension, diabetes mellitus, dyslipidemia (high LDL, low HDL), physical inactivity, abdominal obesity, and a family history of early cardiovascular events. Risk-stratification systems such as SCORE2 integrate these factors to estimate 10-year risk.
Cancer: smoking (lung, bladder, pancreas, larynx), alcohol (liver, esophagus, colon), HPV (cervix, oropharynx), obesity (colon, postmenopausal breast, endometrium, kidney), chronic sun exposure (melanoma, skin carcinomas), and asbestos (mesothelioma). For many cancers, risk factors are now the foundation of primary prevention.
Type 2 diabetes: obesity (especially abdominal), physical inactivity, a first-degree family history, metabolic syndrome, prediabetes, and certain ethnicities. The vast majority of risk factors for type 2 diabetes are modifiable — which makes it one of the most preventable chronic diseases.
ARDS (Acute Respiratory Distress Syndrome): severe pneumonia, sepsis, chest trauma, and aspiration of gastric contents. The LIPS Score (Lung Injury Prediction Score) quantifies the risk of developing ARDS in hospitalized patients with these conditions, allowing preventive surveillance to be intensified.
From Knowledge to Action: The Role of Prevention
Knowing your risk factors is not about worrying: it is about acting. Modifiable factors are the primary target of primary prevention — the kind that intervenes before disease develops.
Early diagnosis — secondary prevention — is most effective when you know whom to focus screening on: people with non-modifiable risk factors (family history, age, genetic predisposition) are those who benefit most from periodic surveillance programs.
A doctor does not assess risk factors in isolation, but in combination: risk stratification integrates several factors to estimate the probability of an event (such as a heart attack, stroke, or cancer) over a given time frame. This makes it possible to personalize recommendations — from how often to screen to whether preventive drug therapy is needed — based on the patient's real profile.
In Clinical Practice
In my clinical practice, I try to explain to patients that knowing your own risk factors is not a sentence or a judgment, but an opportunity. Those who know their risks can act on the modifiable ones and carefully monitor the ones they cannot change. It is the difference between being subject to your own biology and managing it consciously.
A patient who smokes and has a family history of heart attack can quit smoking: in doing so, they eliminate the most powerful modifiable cardiovascular risk factor. A patient who is BRCA1-positive cannot change their genome, but they can choose an intensified surveillance plan that radically changes the prognosis should cancer arise.
FAQ
Does having a risk factor mean I will get sick?
No. A risk factor increases the probability of getting sick, but not the certainty. Millions of smokers never develop lung cancer. And having no risk factors does not guarantee absolute protection. Risk is always probabilistic, never deterministic.
What are the main cardiovascular risk factors?
The main modifiable cardiovascular risk factors are: smoking, hypertension, diabetes mellitus, high cholesterol (especially elevated LDL), physical inactivity, abdominal obesity, and poor diet. The main non-modifiable ones are: age (>45 years in men, >55 in women), male sex, and a family history of early cardiovascular events (father or brother before age 55, mother or sister before age 65).
Are risk factors hereditary?
Some are, some are not. Family history and genetic predispositions (such as familial hypercholesterolemia or BRCA mutations) are hereditary. Most modifiable risk factors — smoking, physical inactivity, diet, obesity — are not genetically determined, although genetic predispositions do influence weight, metabolism, and the stress response. This does not reduce individual responsibility for managing the modifiable factors.
Dr. Marco De Nardin
Medical Doctor, Specialist in Anesthesiology, Intensive Care and Pain Management
Dr. Marco De Nardin is a physician specializing in Anesthesiology, Intensive Care, and Pain Management. He completed his medical degree and specialty training in Italy, where he continues to practice at his private clinics in Mestre (Venice) and Milan. With extensive clinical experience spanning operating rooms, intensive care units, and pain management clinics, Dr. De Nardin brings a unique perspective that bridges acute-care medicine with chronic disease management. His clinical practice focuses on regional anesthesia, ozone therapy, intravenous infusion therapy, and integrative approaches to pain treatment. He is the founder of Med4Care, a medical information platform delivering evidence-based, physician-reviewed health content. Every article published under his name reflects his commitment to making complex medical topics accessible to patients without compromising scientific rigor.